Case 5
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment"
35 yrs female ,came to opd with complaints of swelling in abdomen since 15 days
History of present illness:
Patient was apparently asymptomatic 15 days ago back .
She developed fever which is mild onset ,gradually it is associated with chills and rigor.
Fever has been subsided taking medication.
-she developed abdominal distension 15 days back
-patient has suffered from loss of appetite from 10 days ago
Past history:
-No history of chest pain ,palpitations,cold ,cough
-patient is not suffering with hypertension
⁃ no history of diabetes,epilepsy,TB,tyroid disorder
⁃ Patient had not undergone any surgeries
⁃ Blood transfusion undergone in 2nd pregnancy
PERSONAL HISTORY:
Diet-mixed
Appetite-loss of appetite
Bowel and bladder-irregular
Sleep-normal
Addiction -no addiction
FAMILY HISTORY:
No history of DM/HTN/TB/ asthma/ thyroid
No similar complaints in the family previously
Treatment history: not significant
GENERAL EXAMINATION:
-Patient is conscious,coherent,and cooperative
⁃ pallor present
⁃ No cyanosis
⁃ No icterus
⁃ No clubbing
⁃ No lymphadenopathy
⁃ Malnutrition is present
⁃ Oedema-absent
⁃ No Dehydration
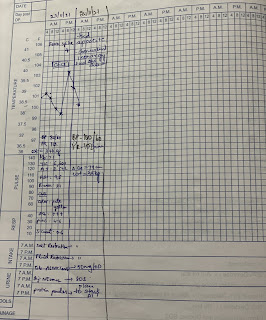
VITALS:
Temp -99.5 C/F
Pulse rate -112/min
Resp rate-18/min
Bp-180/60
Spo2-99%
Systemic examination:
1.cvs-inspection-chest wall is bilateral systemically
Palpation -normal
Auscultation-normal with regular heart beat
S1 S2 heard
No murmurs
2.respiratory system:
Position of trachea-central,normal bilateral air entry,no Av sound
Dyspnea is seen ,expiratory wheeze is position in all area
Breath sound is vascular
3.abdomen:

GI tract /mesentery /peritoneal cavity:
-Large lobulated ascites causing peripheral displacement large bowel loops,free ascites
-mild free ascites
⁃ significant omental thickening
⁃ Mesentric and anterior diaphymatic lymphadenopathy
⁃
4.CNS:
Patient is conscious,
Speech is normal
Neck stiffness is not seen
Cranial nerves,motar system,sensory system is not seen.
Investigation:
















Comments
Post a Comment